
Enlarge / The structure of the human factor VIII. (credit: University of Washington)
Rational drug design seems so promising. So, you know, rational. How could it not work? Here’s the premise:
- 1. Identify a drug that has a desired effect. This is usually done either by screening a library of possible drugs or even of random chemicals, or by actively searching for a molecule hypothesized to be active against a cellular target of interest.
- 2. Figure out how the candidate drug works. What is its target is in the cell? How does it interact with said target?
- 3. Design a drug that optimizes its attraction to the target so that the final drug binds more strongly to its target, or stays bound for longer, or doesn’t accidentally also bind to something else.
Optimizing can be done by tweaking a drug’s interaction with its target: changing its shape, size, or electric charge so that it fits better. These modifications can be designed and assayed on a computer before a drug is synthesized and tested in the real world—first against a drug’s isolated target, then in cultured cells, and then animals. If all those work out, the modified drug may eventually be tested in humans.
The strategy has yielded some spectacular successes, most notably HIV protease inhibitors. But rational drug design is costly, in terms of time, money, materials, and effort. And too often it yields end products that are too toxic to be used pharmacologically, even if they bind their target well.
Read 6 remaining paragraphs | Comments
 Künftige Android-Smartphones mit Google-Lizenz können auch ohne Hangouts in den Handel kommen - die Installation ist künftig nicht mehr zwingend. Stattdessen wird der Videochat Duo eine der vorgeschriebenen Kern-Apps, die im Rahmen der Google-Apps installiert sein müssen. (
Künftige Android-Smartphones mit Google-Lizenz können auch ohne Hangouts in den Handel kommen - die Installation ist künftig nicht mehr zwingend. Stattdessen wird der Videochat Duo eine der vorgeschriebenen Kern-Apps, die im Rahmen der Google-Apps installiert sein müssen. (
 X-Plane 11 ist in Arbeit. Einer der wenigen verbliebenen Flugsimulatoren bekommt ein Update, das vor allem die Grafik verbessern soll. Einen ersten Trailer mit blitzblanken Flugzeugen zeigt Laminar Research bereits, und die Veröffentlichung ist nah. (
X-Plane 11 ist in Arbeit. Einer der wenigen verbliebenen Flugsimulatoren bekommt ein Update, das vor allem die Grafik verbessern soll. Einen ersten Trailer mit blitzblanken Flugzeugen zeigt Laminar Research bereits, und die Veröffentlichung ist nah. ( Der Bundesrat fordert, dass nach 2030 keine Autos mit Verbrennungsmotoren mehr zugelassen werden sollen. Der Beschluss soll parteiübergreifend beschlossen worden sein - und könnte die Verbreitung von emissionsfreien PKW beschleunigen. (
Der Bundesrat fordert, dass nach 2030 keine Autos mit Verbrennungsmotoren mehr zugelassen werden sollen. Der Beschluss soll parteiübergreifend beschlossen worden sein - und könnte die Verbreitung von emissionsfreien PKW beschleunigen. (
 Bisher hat Microsoft seinen Edge-Browser nur dann aktualisiert, wenn auch ein Windows-Update verteilt wurde. Diese Frequenz will der Hersteller jetzt durch Updates über den Windows Store erhöhen. (
Bisher hat Microsoft seinen Edge-Browser nur dann aktualisiert, wenn auch ein Windows-Update verteilt wurde. Diese Frequenz will der Hersteller jetzt durch Updates über den Windows Store erhöhen. ( Da ein Austauschgerät des Galaxy Note 7 unter Verdacht steht, in einem Flugzeug Rauch verursacht zu haben, soll der US-Netzbetreiber AT&T die Verkäufe von Samsungs Top-Smartphone stoppen wollen. Dies wäre ein weiterer schwerer Schlag für Samsung. (
Da ein Austauschgerät des Galaxy Note 7 unter Verdacht steht, in einem Flugzeug Rauch verursacht zu haben, soll der US-Netzbetreiber AT&T die Verkäufe von Samsungs Top-Smartphone stoppen wollen. Dies wäre ein weiterer schwerer Schlag für Samsung. (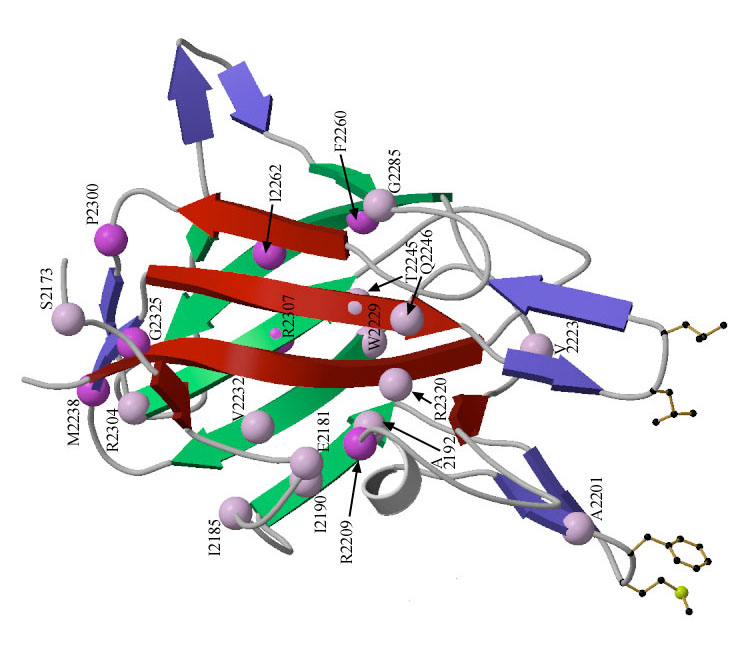{kind=link}
{kind=link}
{kind=link}